‘Opportunistic’ patient poaching by multi-practice chain clinics.
In the context of Covid 19 immunisation program, multi-practice chain clinics are being provided with hundreds more Covid 19 vaccinations per clinic than traditional general practice clinics. This appears to be the case even where the clinics do not have the status of being a respiratory clinic nor are they of significantly greater size compared to peers.
One can only wonder at the underhanded machinations of government-medical clinic dealings that resulted in this asymmetric arrangement which provides large chain clinics with the much sought-after vaccine in higher numbers.
The government website for Covid 19 vaccination information supplies the community with much-needed information on accessible vaccination providers. This of course means patients will be shopping for the 1st/ most available Covid 19 vaccine provider.
This would generally not be a problem and etiquette between general practices means that we would be happy to provide patient information for other clinics providing emergency/one-time services.
However, it appears that large chain clinics for are utilising the opportunity to request medical history summaries be supplied from the patient's traditional provider. Patients are being told to bring a medical summary provided by your usual doctor to enable receiving the covid 19 vaccine.
So far so good you think. Cooperation and effective utilisation of resources in action.
I would like you to pause and take a moment to think about the consequences of a clinic that swallows up hundreds of your patient files. Patient data is dutifully entered into the receiving clinics patient database. The clinic does not differentiate these patients.
Next fortnight as flu vaccine is available and appropriate these patients receive an automated reminder from the receiving clinic to return for their influenza vaccination.
The following week the patients with diabetes receive an automated reminder to return for a diabetes review clinic appointment.
This is not necessarily due to any covert actions on the part of the receiving clinic, one would hope, but is inherent to the automated recall systems they have set up.
Already we are seeing this in action. Our patients being recalled to the chain clinic for provision of routine care and other immunisations. We are only 2 weeks into Covid 19 vaccination rollout. This situation will only accelerate as the supply disparity becomes more evident.
Thus, we are becoming reticent to provide these chain clinics with patient information which will then be incorporated as a full medical history into the receiving clinic without the patient’s directive and consent for transfer of patient care.
This issue will need to be addressed at a GP community level. We need to acknowledge to dire need to accelerate Covid vaccine rollout but come to an agreement on acceptable level of information required to be provided by the patients regular GP and acceptable handling of received information.
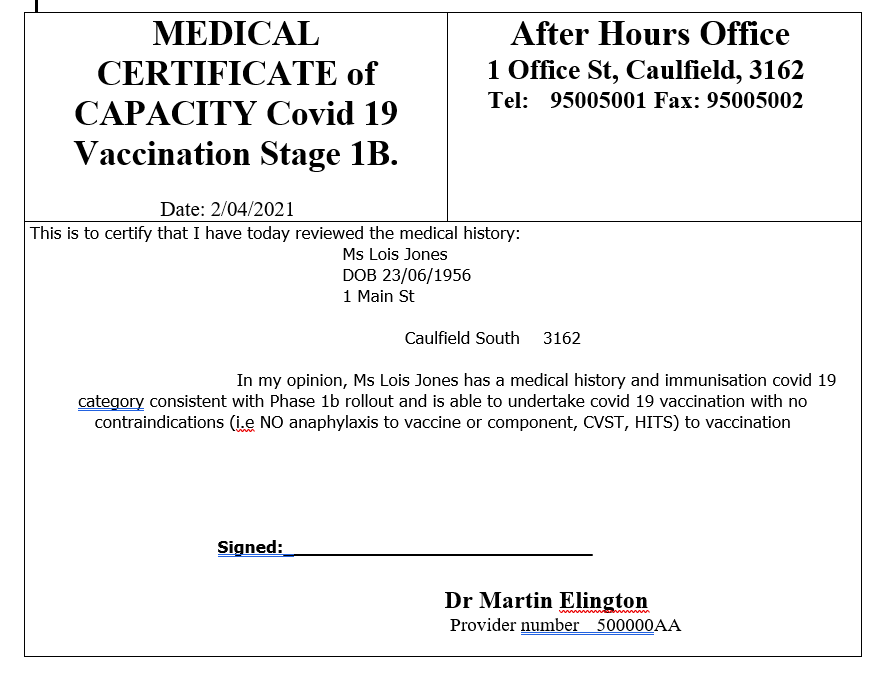
Until this issue is addressed, it may be appropriate to limit information transferred to a certificate of capacity to undergo vaccination covering all relevant requirements of knowledge regarding patient medical profile.